

Introduction:
Approximately 20% of Myelodysplastic Syndromes (MDS) and Chronic Myelomonocytic Leukemia (CMML) are associated with SIAD, but pathophysiological mechanisms underlying this association remain largely unknown and data on somatic mutations are very scarce. Autoreactive T lymphocytes play a major role in SIAD development. The main objective of this study was to investigate the mutational landscape of MDS/CMML associated with SIAD, and its impact on the immunological phenotype of T lymphocytes.
Patients and Methods:
This retrospective study was conducted in the hematology department of Hôpital Saint-Louis, Paris, in all MDS/CMML patients diagnosed between 2012 and 2017, and with a molecular analysis by NGS targeting a panel of 80 genes. MDS/CMML patients with associated SIAD (n= 85, whose diagnosis was based on usual international criteria) were compared with MDS/CMML patients without SIAD (n=319) who constituted the control cohort.
Flow cytometry was performed on peripheral blood samples from 28 MDS/CMML patients (of whom 12/28 had SIAD) and 18 healthy controls, on a BD Fortessa X20 to study CD8+T lymphocytes subsets and the expression of immune checkpoints. Analysis was performed with FlowAI R v1.14.0 and Cytobank website for T cells clustering with unsupervised Citrus algorithm.
Results:
We included 404 MDS/CMML patients (323 MDS, 81 CMML), of whom 85 (21%) had SIAD diagnoses including 35 (34%) inflammatory arthritis, 20 (19%) systemic vasculitis, 16 (15%) autoimmune cytopenias, 15 (14%) connective tissue diseases, 9 (9%) neutrophilic dermatosis, 6 (6%) inflammatory bowel disease, and 3 (3%) unclassified SIAD. Both SIAD and control cohorts were similar in terms of age, levels of cytopenias, MDS/CMML subtypes and cytogenetic features. There was a preponderance of low risk MDS/CMML (85.9% and 82.8% in SIAD and control cohort), and the number of patients with CMML did not differ between the 2 groups (p=0.36). Median follow-up was 32.2 months in the whole cohort. Median overall survival was 95.7 months [60.7 - not estimable] and 101.0 months [70.8 - not estimable] in the control and SIAD cohort respectively (p=0.91).
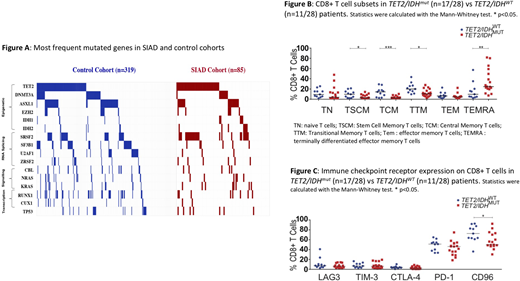
Figure A represents the mutational landscape of MDS/CMML patients for the recurrent mutated genes. Median number of mutations was 2 [1-4] in both cohorts (ns). TET2mutations were found in 39/85 (46%) and 108/319 (34%) patients in the SIAD and control cohorts respectively (p=0.04), and IDH1/2 mutationsin 12/85 (14%) patients in the SIAD cohort vs 14/319 (4%) in the control group (p<0.01). When considering TET2/IDH genes (that act on the same methylation pathway) together, their mutations were more frequent in the SIAD cohort (51/85 (60%) vs 122/319 (38%), p<0.01).
SRSF2 mutations were also more frequent in the SIAD cohort (26/85 (31%) vs 47/319 (15%), p<0.01), but they were correlated with the presence of TET2 or IDH mutations, in both SIAD (p<0.01) and control (p<0.01) cohorts, which could possibly explain the higher frequency of SRSF2 mutations in our SIAD cohort.There was no difference in the rate of mutations in other genes.
Flow cytometry analysis of CD8+ T cells from TET2/IDHmut patients (17/28, 60.7%) showed an increase of the terminally differenciated effector memory T cells (p<0.01) and a reduction of the stem memory (p=0.02), central (p<0.01) and transitional (p=0.01) memory subsets. CD96 is an immune checkpoint that regulates CD8+ T-cell functions, activation and effector responses (Figure B). Interestingly, the proportion of CD8+CD96+T cells was significantly reduced in TET2/IDHmut patients (48.8% vs 71.1% respectively, p<0.05, Figure C), confirmed by unsupervised analysis using the Citrus Algorithm, and suggesting a reduced control against autoimmune reactivity. TET2/IDH mutational status had not impact on the expression of other immune checkpoints.
Discussion
Our study provides an extended mutational landscape of MDS/CMML associated with SIAD, and finds a correlation between TET2/IDH mutations, T lymphocyte imbalance and association with SIAD in those diseases. This correlation could suggest common mechanisms underlying both SIAD and MDS/CMML, and reinforces our observations of a frequent positive effect of Azacytidine (a drug with better response in patients with TET2mutation) on both MDS/CMML and SIAD in patients with both disorders (Fraison, Leuk Res 2016). Further analysis of the functional role of T lymphocytes in those patients is underway.
Clappier:Amgen: Honoraria, Research Funding. Itzykson:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Research Funding; Oncoethix (now Merck): Research Funding; Astellas: Honoraria; Sanofi: Honoraria; BMS (Celgene): Honoraria; Daiichi Sankyo: Honoraria; Jazz Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Honoraria; Amgen: Membership on an entity's Board of Directors or advisory committees; Otsuka Pharma: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Stemline: Membership on an entity's Board of Directors or advisory committees. Mékinian:LFB: Honoraria; CELGENE: Honoraria; CELGENE: Honoraria; SANOFI: Honoraria. Fenaux:BMS: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; Jazz: Honoraria, Research Funding. Ades:jazz: Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Research Funding; takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; novartis: Research Funding; Celgene/BMS: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal